
Glucose-6-Phosphate Dehydrogenase (G6PD) Measurement Using Biosensors by Community-Based Village Malaria Workers and Hospital Laboratory Staff in Cambodia: A Quantitative Study

 , , and
, , and
Abstract
:1. Introduction
1.1. Vivax malaria in Cambodia
1.2. What Is G6PD Deficiency and Why Do We Need a Quantitative Measurement?
2. Materials and Methods
2.1. Roll Out Radical Cure (RORC)
2.2. Deployment of Biosensors in the Hands of Village Malaria Workers
2.3. Data Collection Instruments
2.4. Data Analysis
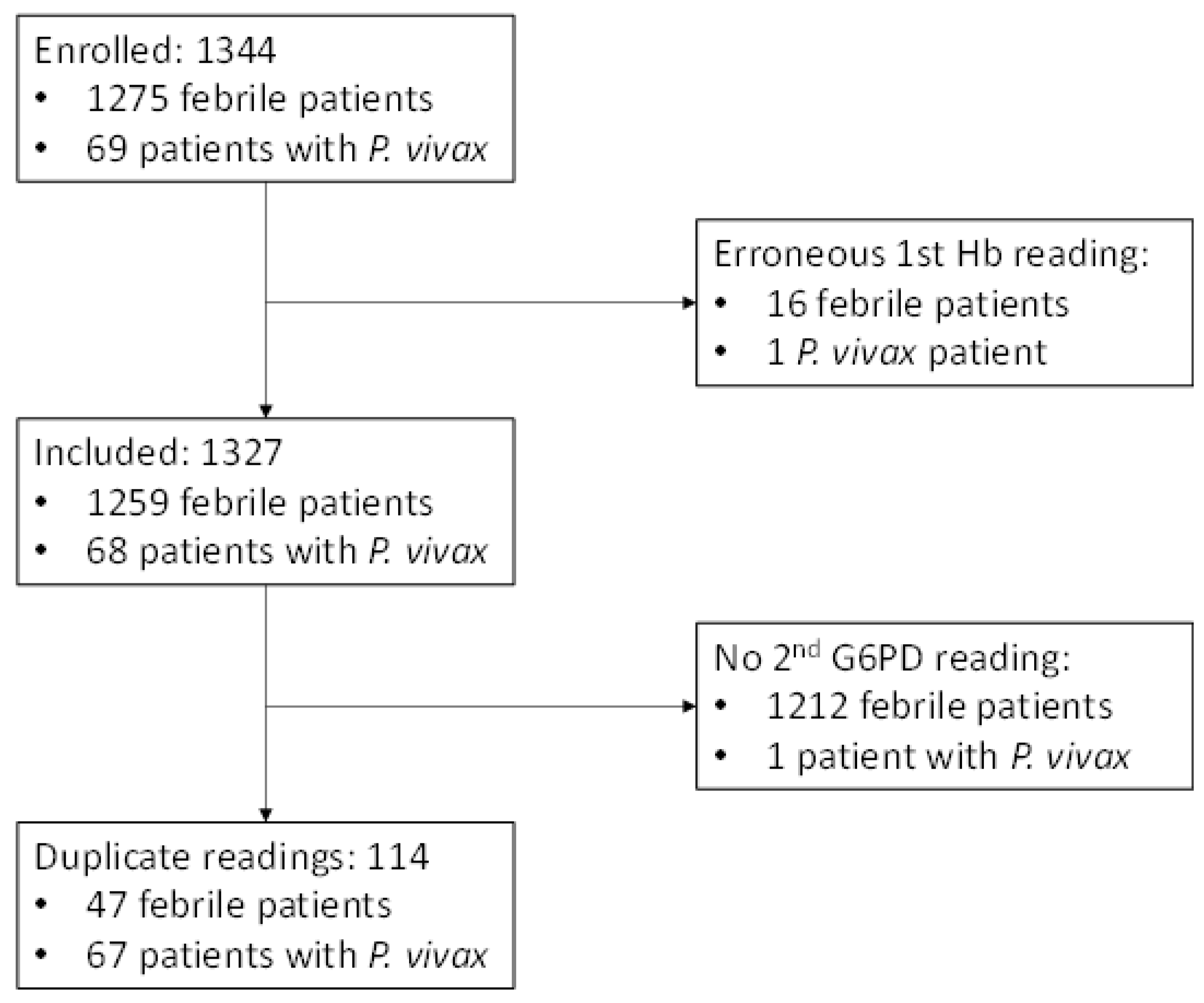
3. Results
3.1. Baseline
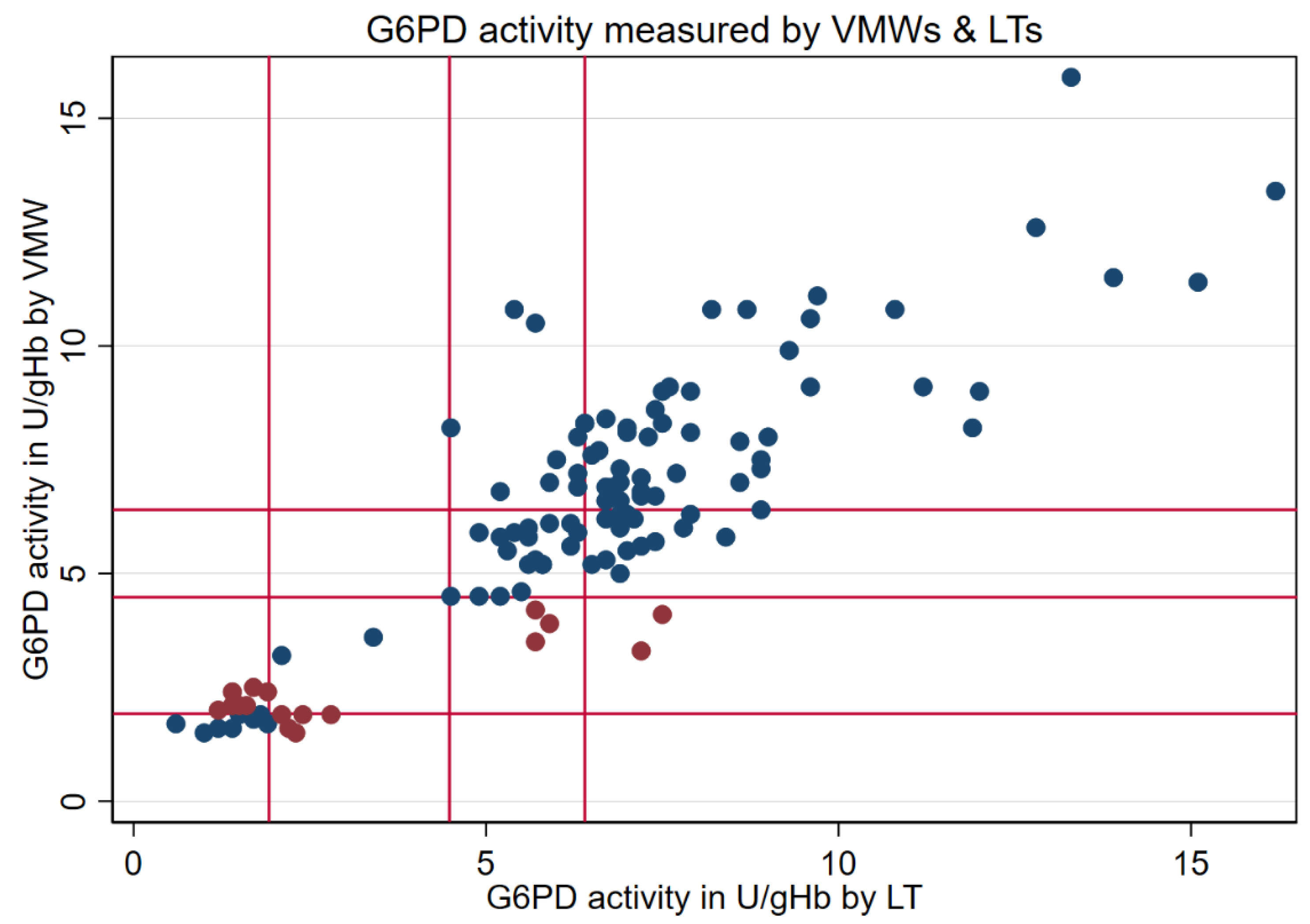
3.2. Paired Results from VMWs and LTs
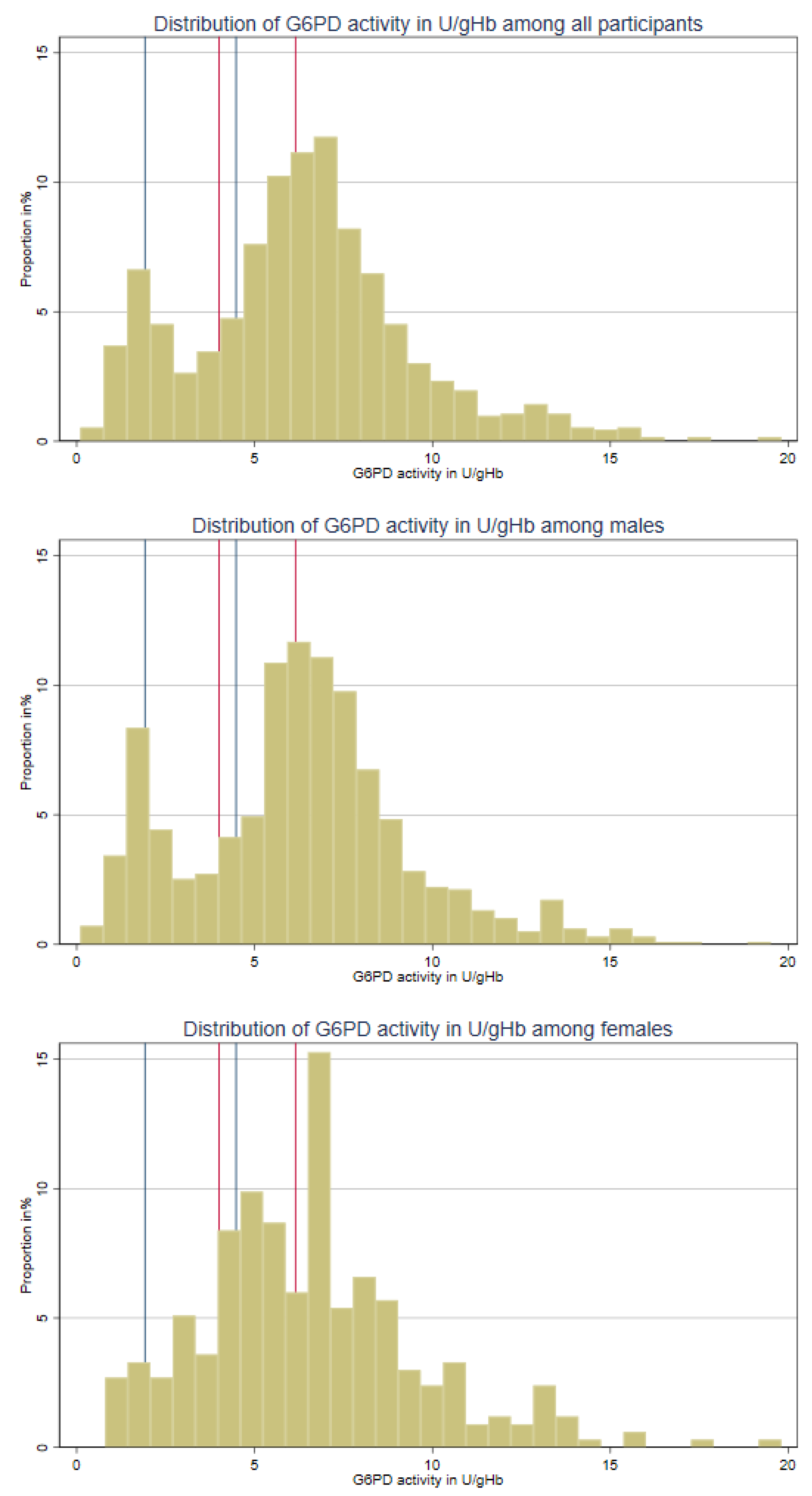
3.3. Distribution of G6PD Activity
3.4. VMWs’ Interpretation of Biosensor Results
3.5. Comparing G6PD Categories: AMM-Based vs. Manufacturer-Recommended
4. Discussion
4.1. VMWs’ Competence in Using the Biosensor and Implications
4.2. G6PD Prevalence and Categorization
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
Appendix A. Case Record Form for Village Malaria Workers and Lab Technicians
| N | Section-I: Socio-Demographics of VMWs/lab Technician | |
| 1. | Unique ID | |
| 2. | Age | |
| 3. | Sex | |
| 4. | Education | |
| 5. | Workplace (e.g., health centre or name of a village) | |
| 6. | Job title | |
| 7. | Years of experience | |
| Section-II: Socio-demographics of participants | ||
| 8. | Unique ID | |
| 9. | Name | |
| 10. | Age | |
| 11. | Sex | |
| 12. | Education (in years) | |
| 13. | Occupation | |
| 14. | Location | |
| Section-III: Clinical history of participants | ||
| 15. | Do you currently have fever? |
|
| 16. | If yes, how long have you got the fever for? | ________days |
| 17. | Have you suffered from malaria in the past? |
|
| 18. | If yes, how long ago was that? | __________days ☐/months ☐/years ☐ |
| 19. | If yes, can you tell me what kind of malaria was it? | Prompt and (use hints):
|
| Section-IV: Biosensor record of patients | ||
| 20. | Machine ID/Code | |
| 21. | Codechip Number | |
| 22. | G6PD (U/g Hb) | |
| 23. | Hemoglobin (Hb) | |
| 24. | Date | |
| 25. | Other (please record as they appear) | |
| 26. | Based on the Biosensor findings, how do you classify G6PD status? |
|
| 27. | What do you advise patients for treatment? | ☐ Chloroquine with
|
References
- Kaehler, N.; Adhikari, B.; Cheah, P.Y.; von Seidlein, L.; Day, N.P.J.; Paris, D.H.; Tanner, M.; Pell, C. Prospects and strategies for malaria elimination in the Greater Mekong Sub-region: A qualitative study. Malar. J. 2019, 18, 203. [Google Scholar] [CrossRef]
- Lek, D.; Callery, J.J.; Nguon, C.; Debackere, M.; Sovannaroth, S.; Tripura, R.; Wojnarski, M.; Piola, P.; Khean, S.T.; Manion, K.; et al. Tools to accelerate falciparum malaria elimination in Cambodia: A meeting report. Malar. J. 2020, 19, 151. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Accelerating Malaria Elimination in the Greater Mekong. 2022. Available online: https://apps.who.int/iris/rest/bitstreams/1413368/retrieve (accessed on 17 March 2022).
- Clinton Health Initiative (CHAI). G6PD Testing in Cambodia and Laos—Piloting and Implementation. 2020. Available online: https://www.vivaxmalaria.org/sites/p-vivax/files/content/attachments/2021-07-21/G6PD%20POC%20implementation_Cambodia%20and%20Laos%20experiences.pdf (accessed on 27 July 2022).
- Centre National de Malariologie (CNM). Malaria Infiormation System. 2022. Available online: https://mis.cnm.gov.kh/ (accessed on 18 June 2022).
- Adhikari, B.; Awab, G.R.; von Seidlein, L. Rolling out the radical cure for vivax malaria in Asia: A qualitative study among policy makers and stakeholders. Malar. J. 2021, 20, 164. [Google Scholar] [CrossRef] [PubMed]
- John, G.K.; Douglas, N.M.; von Seidlein, L.; Nosten, F.; Baird, J.K.; White, N.J.; Price, R.N. Primaquine radical cure of Plasmodium vivax: A critical review of the literature. Malar. J. 2012, 11, 280. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.R.; O’Malley, G.F. Glucose 6 Phosphate Dehydrogenase Deficiency. In StatPearls; StatPearls: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK470315/ (accessed on 12 February 2023).
- Maurya, P.K.; Kumar, P.; Chandra, P. Age-dependent detection of erythrocytes glucose-6-phosphate dehydrogenase and its correlation with oxidative stress. Arch. Physiol. Biochem. 2016, 122, 61–66. [Google Scholar] [CrossRef]
- Cappellini, M.D.; Fiorelli, G. Glucose-6-phosphate dehydrogenase deficiency. Lancet 2008, 371, 64–74. [Google Scholar] [CrossRef]
- LaRue, N.; Kahn, M.; Murray, M.; Leader, B.T.; Bansil, P.; McGray, S.; Kalnoky, M.; Zhang, H.; Huang, H.; Jiang, H.; et al. Comparison of quantitative and qualitative tests for glucose-6-phosphate dehydrogenase deficiency. Am. J. Trop. Med. Hyg. 2014, 91, 854–861. [Google Scholar] [CrossRef]
- Gomez-Manzo, S.; Marcial-Quino, J.; Vanoye-Carlo, A.; Serrano-Posada, H.; Ortega-Cuellar, D.; Gonzalez-Valdez, A.; Castillo-Rodriguez, R.A.; Hernandez-Ochoa, B.; Sierra-Palacios, E.; Rodriguez-Bustamante, E.; et al. Glucose-6-Phosphate Dehydrogenase: Update and Analysis of New Mutations around the World. Int. J. Mol. Sci. 2016, 17, 2069. [Google Scholar] [CrossRef]
- Domingo, G.J.; Advani, N.; Satyagraha, A.W.; Sibley, C.H.; Rowley, E.; Kalnoky, M.; Cohen, J.; Parker, M.; Kelley, M. Addressing the gender-knowledge gap in glucose-6-phosphate dehydrogenase deficiency: Challenges and opportunities. Int. Health 2019, 11, 7–14. [Google Scholar] [CrossRef]
- Pfeffer, D.A.; Ley, B.; Howes, R.E.; Adu, P.; Alam, M.S.; Bansil, P.; Boum, Y., 2nd; Brito, M.; Charoenkwan, P.; Clements, A.; et al. Quantification of glucose-6-phosphate dehydrogenase activity by spectrophotometry: A systematic review and meta-analysis. PLoS Med. 2020, 17, e1003084. [Google Scholar] [CrossRef]
- Henriques, G.; Phommasone, K.; Tripura, R.; Peto, T.J.; Raut, S.; Snethlage, C.; Sambo, I.; Sanann, N.; Nguon, C.; Adhikari, B.; et al. Comparison of glucose-6 phosphate dehydrogenase status by fluorescent spot test and rapid diagnostic test in Lao PDR and Cambodia. Malar. J. 2018, 17, 243. [Google Scholar] [CrossRef]
- Von Seidlein, L.; Auburn, S.; Espino, F.; Shanks, D.; Cheng, Q.; McCarthy, J.; Baird, K.; Moyes, C.; Howes, R.; Menard, D.; et al. Review of key knowledge gaps in glucose-6-phosphate dehydrogenase deficiency detection with regard to the safe clinical deployment of 8-aminoquinoline treatment regimens: A workshop report. Malar. J. 2013, 12, 112. [Google Scholar] [CrossRef]
- Kitchakarn, S.; Lek, D.; Thol, S.; Hok, C.; Saejeng, A.; Huy, R.; Chinanonwait, N.; Thimasarn, K.; Wongsrichanalai, C. Implementation of G6PD testing and primaquine for P. vivax radical cure: Operational perspectives from Thailand and Cambodia. WHO South East Asia J. Public Health 2017, 6, 60–68. [Google Scholar] [CrossRef]
- Adhikari, B.; Tripura, R.; Dysoley, L.; Callery, J.J.; Peto, T.J.; Heng, C.; Vanda, T.; Simvieng, O.; Cassidy-Seyoum, S.; Ley, B.; et al. Glucose 6 Phosphate Dehydrogenase (G6PD) quantitation using biosensors at the point of first contact: A mixed method study in Cambodia. Malar. J. 2022, 21, 282. [Google Scholar] [CrossRef]
- Domingo, G.J.; Satyagraha, A.W.; Anvikar, A.; Baird, K.; Bancone, G.; Bansil, P.; Carter, N.; Cheng, Q.; Culpepper, J.; Eziefula, C.; et al. G6PD testing in support of treatment and elimination of malaria: Recommendations for evaluation of G6PD tests. Malar. J. 2013, 12, 391. [Google Scholar] [CrossRef]
- Ley, B.; Bancone, G.; von Seidlein, L.; Thriemer, K.; Richards, J.S.; Domingo, G.J.; Price, R.N. Methods for the field evaluation of quantitative G6PD diagnostics: A review. Malar. J. 2017, 16, 361. [Google Scholar] [CrossRef]
- Ley, B.; Alam, M.S.; O’Donnell, J.J.; Hossain, M.S.; Kibria, M.G.; Jahan, N.; Khan, W.A.; Thriemer, K.; Chatfield, M.D.; Price, R.N.; et al. A Comparison of Three Quantitative Methods to Estimate G6PD Activity in the Chittagong Hill Tracts, Bangladesh. PLoS ONE 2017, 12, e0169930. [Google Scholar] [CrossRef]
- Adhikari, B.; Tripura, R.; Peto, T.J.; Callery, J.J.; von Seidlein, L.; Dysoley, L.; Dondorp, A.M. Village malaria workers for the community-based management of vivax malaria. Lancet Reg. Health Southeast Asia 2023, 9, 100128. [Google Scholar] [CrossRef]
- Pal, S.; Bansil, P.; Bancone, G.; Hrutkay, S.; Kahn, M.; Gornsawun, G.; Penpitchaporn, P.; Chu, C.S.; Nosten, F.; Domingo, G.J. Evaluation of a Novel Quantitative Test for Glucose-6-Phosphate Dehydrogenase Deficiency: Bringing Quantitative Testing for Glucose-6-Phosphate Dehydrogenase Deficiency Closer to the Patient. Am. J. Trop. Med. Hyg. 2019, 100, 213–221. [Google Scholar] [CrossRef]
- Pal, S.; Myburgh, J.; Bansil, P.; Hann, A.; Robertson, L.; Gerth-Guyette, E.; Ambler, G.; Bizilj, G.; Kahn, M.; Zobrist, S.; et al. Reference and point-of-care testing for G6PD deficiency: Blood disorder interference, contrived specimens, and fingerstick equivalence and precision. PLoS ONE 2021, 16, e0257560. [Google Scholar] [CrossRef]
- Bancone, G.; Gilder, M.E.; Win, E.; Gornsawun, G.; Penpitchaporn, P.; Moo, P.K.; Archasuksan, L.; Wai, N.S.; Win, S.; Aung, K.K.; et al. Technical evaluation and usability of a quantitative G6PD POC test in cord blood: A mixed-methods study in a low-resource setting. BMJ Open 2022, 12, e066529. [Google Scholar] [CrossRef] [PubMed]
- Gerth-Guyette, E.; Adissu, W.; Brito, M.; Garbin, E.; Macedo, M.; Sharma, A.; Das, S.; Lacerda, M.V.G.; Pereira, D.; Talukdar, A.; et al. Usability of a point-of-care diagnostic to identify glucose-6-phosphate dehydrogenase deficiency: A multi-country assessment of test label comprehension and results interpretation. Malar. J. 2021, 20, 307. [Google Scholar] [CrossRef] [PubMed]
- Engel, N.; Ghergu, C.; Matin, M.A.; Kibria, M.G.; Thriemer, K.; Price, R.N.; Ding, X.C.; Howes, R.E.; Ley, B.; Incardona, S.; et al. Implementing radical cure diagnostics for malaria: User perspectives on G6PD testing in Bangladesh. Malar. J. 2021, 20, 217. [Google Scholar] [CrossRef] [PubMed]
- Zobrist, S.; Brito, M.; Garbin, E.; Monteiro, W.M.; Clementino Freitas, S.; Macedo, M.; Soares Moura, A.; Advani, N.; Kahn, M.; Pal, S.; et al. Evaluation of a point-of-care diagnostic to identify glucose-6-phosphate dehydrogenase deficiency in Brazil. PLoS Negl. Trop. Dis. 2021, 15, e0009649. [Google Scholar] [CrossRef] [PubMed]
- Plasmodium vivax Information Hub. Quantitative G6PD Diagnostics Followed by Treatment Decision for Vivax Malaria: How Do Village Malaria Workers Perform? 2021. Available online: https://www.vivaxmalaria.org/quantitative-g6pd-diagnostics-followed-by-treatment-decision-for-vivax-malaria-how-do-village (accessed on 11 June 2022).
- Thriemer, K.; Degaga, T.S.; Alam, M.S.; Adhikari, B.; Tripura, R.; Hossain, M.S.; Christian, M.; Ghanchi, N.; Mnjala, H.; Weston, S.; et al. Adapting international clinical trials during COVID-19 and beyond. Clin. Trials 2023, 17407745231154215. online ahead of print. [Google Scholar] [CrossRef]
- Satyagraha, A.W.; Sadhewa, A.; Baramuli, V.; Elvira, R.; Ridenour, C.; Elyazar, I.; Noviyanti, R.; Coutrier, F.N.; Harahap, A.R.; Baird, J.K. G6PD deficiency at Sumba in Eastern Indonesia is prevalent, diverse and severe: Implications for primaquine therapy against relapsing Vivax malaria. PLoS Negl. Trop. Dis. 2015, 9, e0003602. [Google Scholar] [CrossRef]
- Ley, B.; Alam, M.S.; Satyagraha, A.W.; Phru, C.S.; Thriemer, K.; Tadesse, D.; Shibiru, T.; Hailu, A.; Kibria, M.G.; Hossain, M.S. Variation in Glucose-6-Phosphate Dehydrogenase activity following acute malaria. PLoS Negl. Trop. Dis. 2022, 16, e0010406. [Google Scholar] [CrossRef]
- Alam, M.; Kibria, M.; Jahan, N.; Thriemer, K.; Hossain, M.; Douglas, N.; Phru, C.S.; Khan, W.A.; Price, R.N.; Ley, B. Field evaluation of quantitative point of care diagnostics to measure glucose-6-phosphate dehydrogenase activity. PLoS ONE 2018, 13, 206331. [Google Scholar] [CrossRef]
- Mbanefo, E.C.; Ahmed, A.M.; Titouna, A.; Elmaraezy, A.; Trang, N.T.; Phuoc Long, N.; Hoang Anh, N.; Diem Nghi, T.; The Hung, B.; Van Hieu, M.; et al. Association of glucose-6-phosphate dehydrogenase deficiency and malaria: A systematic review and meta-analysis. Sci. Rep. 2017, 7, 45963. [Google Scholar] [CrossRef]
- Awab, G.R.; Aaram, F.; Jamornthanyawat, N.; Suwannasin, K.; Pagornrat, W.; Watson, J.A.; Woodrow, C.J.; Dondorp, A.M.; Day, N.P.; Imwong, M.; et al. Protective effect of Mediterranean-type glucose-6-phosphate dehydrogenase deficiency against Plasmodium vivax malaria. eLife 2021, 10, e62448. [Google Scholar] [CrossRef]
- Kheang, S.T.; Ridley, R.; Ngeth, E.; Ir, P.; Ngor, P.; Sovannaroth, S.; Lek, D.; Phon, S.; Kak, N.; Yeung, S. G6PD testing and radical cure for Plasmodium vivax in Cambodia: A mixed methods implementation study. PLoS ONE 2022, 17, e0275822. [Google Scholar] [CrossRef]
- Soremekun, S.; Kasteng, F.; Lingam, R.; Vassall, A.; Kertho, E.; Settumba, S.; Etou, P.L.; Nanyonjo, A.; Ten Asbroek, G.; Kallander, K.; et al. Variation in the quality and out-of-pocket cost of treatment for childhood malaria, diarrhoea, and pneumonia: Community and facility based care in rural Uganda. PLoS ONE 2018, 13, e0200543. [Google Scholar] [CrossRef]
- Yeboah-Antwi, K.; Pilingana, P.; Macleod, W.B.; Semrau, K.; Siazeele, K.; Kalesha, P.; Hamainza, B.; Seidenberg, P.; Mazimba, A.; Sabin, L.; et al. Community case management of fever due to malaria and pneumonia in children under five in Zambia: A cluster randomized controlled trial. PLoS Med. 2010, 7, e1000340. [Google Scholar] [CrossRef]
- Kalyango, J.N.; Rutebemberwa, E.; Karamagi, C.; Mworozi, E.; Ssali, S.; Alfven, T.; Peterson, S. High adherence to antimalarials and antibiotics under integrated community case management of illness in children less than five years in eastern Uganda. PLoS ONE 2013, 8, e60481. [Google Scholar] [CrossRef]
- Christopher, J.B.; Le May, A.; Lewin, S.; Ross, D.A. Thirty years after Alma-Ata: A systematic review of the impact of community health workers delivering curative interventions against malaria, pneumonia and diarrhoea on child mortality and morbidity in sub-Saharan Africa. Hum. Resour. Health 2011, 9, 27. [Google Scholar] [CrossRef]
- McCord, G.C.; Liu, A.; Singh, P. Deployment of community health workers across rural sub-Saharan Africa: Financial considerations and operational assumptions. Bull. World Health Organ. 2013, 91, 244–253b. [Google Scholar] [CrossRef]
- Vaughan, K.; Kok, M.C.; Witter, S.; Dieleman, M. Costs and cost-effectiveness of community health workers: Evidence from a literature review. Hum. Resour. Health 2015, 13, 71. [Google Scholar] [CrossRef]
- WHO. The ‘Last Mile’ of Malaria Elimination in Cambodia. 2022. Available online: https://www.who.int/news-room/feature-stories/detail/the-last-mile-of-malaria-elimination-in-cambodia (accessed on 27 December 2022).
- Mitchell, M.; Kan, L. Digital Technology and the Future of Health Systems. Health Syst. Reform. 2019, 5, 113–120. [Google Scholar] [CrossRef]
- Barts Health Knowledge and Library Services. Clinical Decision Support Tools. 2022. Available online: https://bartshealth-nhs.libguides.com/CDS (accessed on 22 December 2022).
- Kawamoto, K.; Houlihan, C.A.; Balas, E.A.; Lobach, D.F. Improving clinical practice using clinical decision support systems: A systematic review of trials to identify features critical to success. BMJ 2005, 330, 765. [Google Scholar] [CrossRef]
- Bright, T.J.; Wong, A.; Dhurjati, R.; Bristow, E.; Bastian, L.; Coeytaux, R.R.; Samsa, G.; Hasselblad, V.; Williams, J.W.; Musty, M.D.; et al. Effect of clinical decision-support systems: A systematic review. Ann. Intern. Med. 2012, 157, 29–43. [Google Scholar] [CrossRef]
- Matsuoka, H.; Nguon, C.; Kanbe, T.; Jalloh, A.; Sato, H.; Yoshida, S.; Hirai, M.; Arai, M.; Socheat, D.; Kawamoto, F. Glucose-6-phosphate dehydrogenase (G6PD) mutations in Cambodia: G6PD Viangchan (871G>A) is the most common variant in the Cambodian population. J. Hum. Genet. 2005, 50, 468–472. [Google Scholar] [CrossRef] [PubMed]
- Bancone, G.; Menard, D.; Khim, N.; Kim, S.; Canier, L.; Nguong, C.; Phommasone, K.; Mayxay, M.; Dittrich, S.; Vongsouvath, M.; et al. Molecular characterization and mapping of glucose-6-phosphate dehydrogenase (G6PD) mutations in the Greater Mekong Subregion. Malar. J. 2019, 18, 20. [Google Scholar] [CrossRef] [PubMed]
- Ley, B.; Winasti Satyagraha, A.; Kibria, M.G.; Armstrong, J.; Bancone, G.; Bei, A.K.; Bizilj, G.; Brito, M.; Ding, X.C.; Domingo, G.J.; et al. Repeatability and reproducibility of a handheld quantitative G6PD diagnostic. PLoS Negl. Trop. Dis. 2022, 16, e0010174. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | LTs (n = 5) | VMWs (n = 28) | |
|---|---|---|---|
| Number (%) | Number (%) | p-Value | |
| Age group | Median = 42 years (IQR = 36–51.5) | ||
| ≤40 years | 2 (40) | 9 (32.1) | 0.55 |
| ≥41 years | 3 (60) | 19 (67.9) | |
| Sex | |||
| Female | 1 (20) | 16 (57.1) | 0.02 |
| Male | 4 (80) | 12 (42.9) | |
| Education | Median = 7 years (IQR = 6–9) | ||
| ≤6 years | 1 (20) | 9 (32.1) | 0.51 |
| ≥7 years | 4 (80) | 19 (67.9) | |
| Experience | Median = 6 years (IQR = 3–6) | ||
| ≤5 years | 2 (40) | 13 (46.4) | 0.5 |
| ≥6 years | 3 (60) | 15 (53.6) | |
| Characteristics of Participants | RDT-Negative Patients (n = 1275) | Vivax Patients (n = 69) | |
|---|---|---|---|
| Number (%) | Number (%) | p-Value | |
| Age (Years) | |||
| Median (IQR) | 32 (24–42) | 22 (18–33) | <0.001 |
| Sex | |||
| Male | 937 (73.5) | 65 (94.2) | |
| Female | 338 (26.5) | 4 (5.8) | <0.001 |
| Education in years | |||
| Median (IQR) | 5 (7–3) | 5 (7–3) | 0.570 |
| Occupation | |||
| Farmer | 1199 (94) | 56 (81.2) | <0.001 |
| Other | 76 (6) | 13 (18.8) | |
| Do you currently have fever? | |||
| Yes * | 1235 (96.9) | 64 (92.8) | |
| No | 37 (2.9) | 5 (7.2) | |
| Other | 3 (0.2) | 0 (0.0) | 0.150 |
| Fever in days | |||
| Median (IQR) | 2 (2–3) | 3 (2–3) | <0.001 |
| Have you suffered from malaria in the past (entire lifetime)? | |||
| Yes ** | 848 (66.5) | 51 (73.9) | |
| No | 427 (33.5) | 18 (26.1) | 0.230 |
| If you had malaria in the past what kind of malaria was it? | |||
| Falciparum | 181 (22) | 1 (2) | |
| Vivax | 643 (78) | 49 (98) | <0.001 |
| LTs | |||||
|---|---|---|---|---|---|
| G6PD Category (AMM%) | Normal | Intermediate | Deficient | Total | |
| VMWs | Normal (>70%) | 87 (75.7) | 0 (0.0) | 0 (0.0) | 87 (76.3) |
| Intermediate (30 to 70%) | 5 (4.4) | 2 (1.7) | 7 (6.1) | 14 (12.3) | |
| Deficient (≤30%) | 0 (0.0) | 5 (4.4) | 8 (7.0) | 13 (11.4) | |
| Total | 92 (80.7) | 7 (6.1) | 15 (13.2) | 114 (100.2) | |
| G6PD Category | Based on AMM (U/g Hb) | Based on Field Implementation * (U/g Hb) | Based on Manufacturer’s Recommendation (U/g Hb) |
|---|---|---|---|
| Deficient (≤30%) | ≤1.9 | ≤2.6 | ≤4.0 |
| Intermediate (30% to 70%) | >1.9 to 4.5 | >2.6 to 6.0 | >4.0 to 6.0 |
| Normal (>70%) | >4.5 | >6.0 | >6.0 |
| Category | Men (%) | Women (%) | Total (%) |
|---|---|---|---|
| RDT-negative patients | |||
| ≥70% | 697 (75.0) | 247 (74.9) | 944 (75.0) |
| ≥30% to <70% | 124 (13.4) | 67 (20.3) | 191 (15.2) |
| <30% | 108 (11.6) | 16 (4.9) | 124 (9.9) |
| Total | 929 (100.0) | 330 (100.0) | 1259 (100.0) |
| Parasitaemic (Vivax patients) | |||
| ≥70% | 51 (79.7) | 3 (75.0) | 54 (79.4) |
| ≥30% to <70% | 6 (9.4) | 0 (0.0) | 6 (8.8) |
| <30% | 7 (10.9) | 1 (25.0) | 8 (11.8) |
| Total | 64 (100.0) | 4 (100.0) | 68 (100.0) |
| Categorization by VMWs | |||||
|---|---|---|---|---|---|
| Category | Normal | Intermediate | Deficient | Total (%) | |
| Calculated G6PD category * | Normal (%) | 607 (82.0) | 102 (13.8) | 31 (4.2) | 740 (55.9) |
| Intermediate (%) | 61 (15.5) | 217 (55.1) | 116 (29.4) | 394 (29.7) | |
| Deficient (%) | 9 (4.7) | 6 (3.1) | 176 (92.2) | 191 (14.4) | |
| Total (%) | 677 (51.1) | 325 (24.5) | 323 (24.4) | 1325 (100.0) | |
| G6PD Category Based on Local AMM | |||||
|---|---|---|---|---|---|
| G6PD category based on manufacturer’s recommendation | Category | Normal | Intermediate | Deficient | Total (%) |
| Normal (%) | 713 (100.0) | 0 (0.0) | 0 (0.0) | 713 (53.7) | |
| Intermediate (%) | 285 (86.6) | 44 (13.4) | 0 (0.0) | 329 (24.8) | |
| Deficient (%) | 0 (0.0) | 153 (53.7) | 132 (46.3) | 285 (21.5) | |
| Total (%) | 998 (75.2) | 197 (14.4) | 132 (10.0) | 1327 (100.0) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adhikari, B.; Tripura, R.; Dysoley, L.; Peto, T.J.; Callery, J.J.; Heng, C.; Vanda, T.; Simvieng, O.; Cassidy-Seyoum, S.; Thriemer, K.; et al. Glucose-6-Phosphate Dehydrogenase (G6PD) Measurement Using Biosensors by Community-Based Village Malaria Workers and Hospital Laboratory Staff in Cambodia: A Quantitative Study. Pathogens 2023, 12, 400. https://doi.org/10.3390/pathogens12030400
Adhikari B, Tripura R, Dysoley L, Peto TJ, Callery JJ, Heng C, Vanda T, Simvieng O, Cassidy-Seyoum S, Thriemer K, et al. Glucose-6-Phosphate Dehydrogenase (G6PD) Measurement Using Biosensors by Community-Based Village Malaria Workers and Hospital Laboratory Staff in Cambodia: A Quantitative Study. Pathogens. 2023; 12(3):400. https://doi.org/10.3390/pathogens12030400
Chicago/Turabian StyleAdhikari, Bipin, Rupam Tripura, Lek Dysoley, Thomas J. Peto, James J. Callery, Chhoeun Heng, Thy Vanda, Ou Simvieng, Sarah Cassidy-Seyoum, Kamala Thriemer, and et al. 2023. "Glucose-6-Phosphate Dehydrogenase (G6PD) Measurement Using Biosensors by Community-Based Village Malaria Workers and Hospital Laboratory Staff in Cambodia: A Quantitative Study" Pathogens 12, no. 3: 400. https://doi.org/10.3390/pathogens12030400