
Vitamin D Deficiency and Its Association with Iron Deficiency in African Children

 , , , , , , , , add
Show full author list
, , , , , , , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Laboratory Assays
2.3. Definitions
2.4. Statistical Analyses
3. Results
3.1. Characteristics of Study Participants
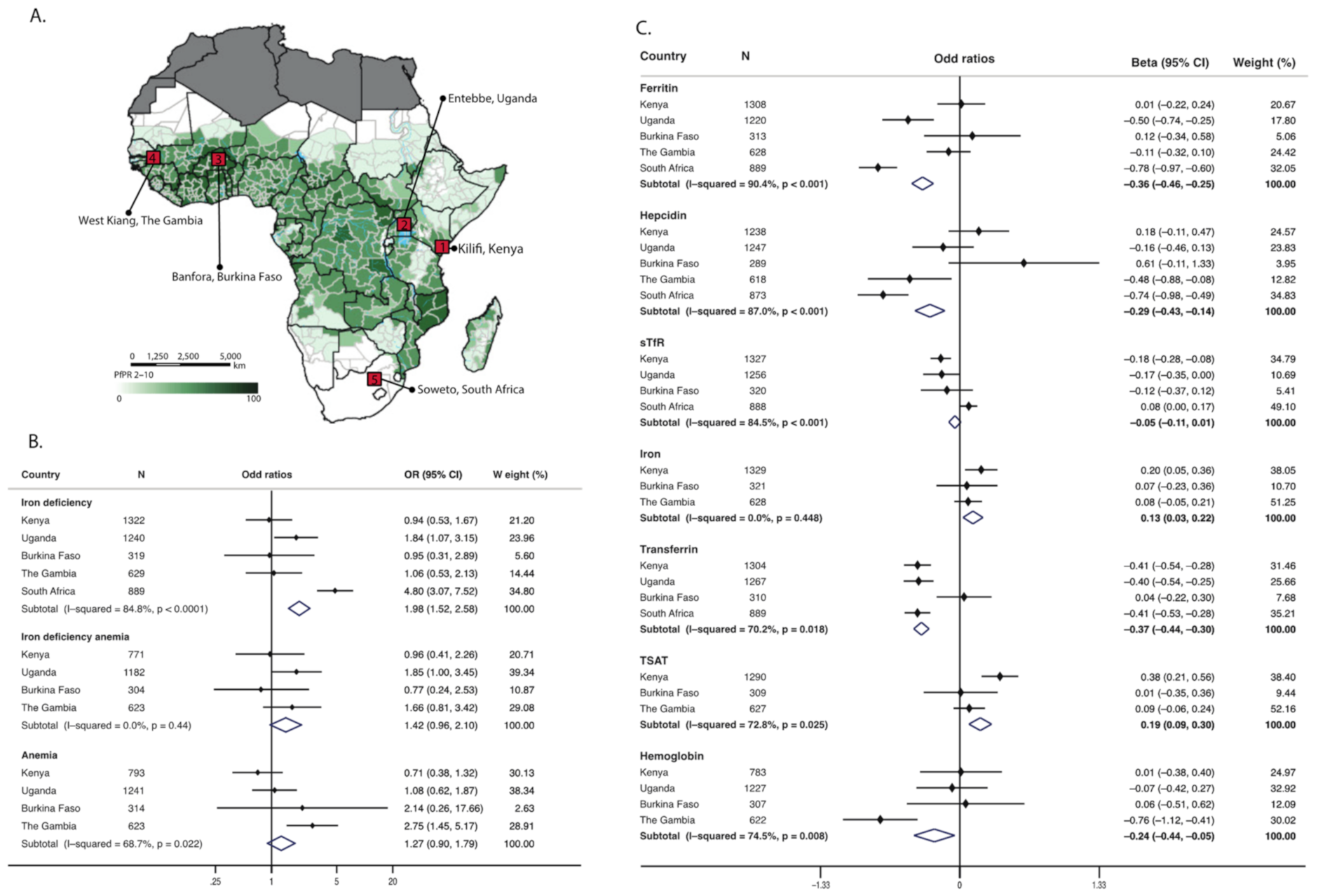
3.2. Vitamin D Status Is Associated with Iron Deficiency
3.3. Vitamin D Status Influences Individual Markers of Iron Status
3.4. Effects of Inflammation and Malaria on Vitamin D and Iron Status
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Kassebaum, N.J. The Global Burden of Anemia. Hematol. Oncol. Clin. North Am. 2016, 30, 247–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mogire, R.M.; Mutua, A.; Kimita, W.; Kamau, A.; Bejon, P.; Pettifor, J.M.; Adeyemo, A.; Williams, T.N.; Atkinson, S.H. Prevalence of vitamin D deficiency in Africa: A systematic review and meta-analysis. Lancet Glob. Health 2020, 8, e134–e142. [Google Scholar] [CrossRef] [Green Version]
- Muriuki, J.M.; Mentzer, A.J.; Webb, E.L.; Morovat, A.; Kimita, W.; Ndungu, F.M.; Macharia, A.W.; Crane, R.J.; Berkley, J.A.; Lule, S.A.; et al. Estimating the burden of iron deficiency among African children. BMC Med. 2020, 18, 31. [Google Scholar] [CrossRef] [Green Version]
- Bacchetta, J.; Zaritsky, J.J.; Sea, J.L.; Chun, R.F.; Lisse, T.S.; Zavala, K.; Nayak, A.; Wesseling-Perry, K.; Westerman, M.; Hollis, B.W.; et al. Suppression of iron-regulatory hepcidin by vitamin D. J. Am. Soc. Nephrol. 2014, 25, 564–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zughaier, S.M.; Alvarez, J.A.; Sloan, J.H.; Konrad, R.J.; Tangpricha, V. The role of vitamin D in regulating the iron-hepcidin-ferroportin axis in monocytes. J. Clin. Transl. Endocrinol. 2014, 1, e19–e25. [Google Scholar] [CrossRef] [PubMed]
- Katsumata, S.; Katsumata, R.; Matsumoto, N.; Inoue, H.; Takahashi, N.; Uehara, M. Iron deficiency decreases renal 25-hydroxyvitamin D3-1α-hydroxylase activity and bone formation in rats. BMC Nutr. 2016, 2, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Clinkenbeard, E.L.; Farrow, E.G.; Summers, L.J.; Cass, T.A.; Roberts, J.L.; Bayt, C.A.; Lahm, T.; Albrecht, M.; Allen, M.R.; Peacock, M.; et al. Neonatal iron deficiency causes abnormal phosphate metabolism by elevating FGF23 in normal and ADHR mice. J. Bone Miner. Res. 2014, 29, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Perwad, F.; Zhang, M.Y.; Tenenhouse, H.S.; Portale, A.A. Fibroblast growth factor 23 impairs phosphorus and vitamin D metabolism in vivo and suppresses 25-hydroxyvitamin D-1alpha-hydroxylase expression in vitro. Am. J. Physiol. Renal Physiol. 2007, 293, F1577–F1583. [Google Scholar] [CrossRef] [Green Version]
- Azizi-Soleiman, F.; Vafa, M.; Abiri, B.; Safavi, M. Effects of Iron on Vitamin D Metabolism: A Systematic Review. Int. J. Prev. Med. 2016, 7, 126. [Google Scholar] [CrossRef]
- Snow, R.W.; Sartorius, B.; Kyalo, D.; Maina, J.; Amratia, P.; Mundia, C.W.; Bejon, P.; Noor, A.M. The prevalence of Plasmodium falciparum in sub-Saharan Africa since 1900. Nature 2017, 550, 515–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houghton, L.A.; Brown, R.C.; Beaumont, S.; Jennings, S.; Bailey, K.B.; Haszard, J.J.; Erhardt, J.; Daniels, L.; Gibson, R.S. Micronutrient status differs among Maasai and Kamba preschoolers in a supplementary feeding programme in Kenya. Matern. Child Nutr. 2019, 15, e12805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulling, P.M.; Olson, K.C.; Olson, T.L.; Feith, D.J.; Loughran, T.P.J. Vitamin D in hematological disorders and malignancies. Eur. J. Haematol. 2017, 98, 187–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aucella, F.; Gatta, G.; Vigilante, M.; Scalzulli, R.P.; Mantuano, S.; Carotenuto, M.; Stallone, C. [Increased in vitro and ex vivo proliferation of erythroid precursors induced by calcitriol in chronic renal failure. Synergistic effect with rHuEPO]. G. Ital. Nefrol. 2002, 19, 137–142. [Google Scholar] [PubMed]
- Wu, W.; Fan, H.; Jiang, Y.; Liao, L.; Li, L.; Zhao, J.; Zhang, H.; Shrestha, C.; Xie, Z. Regulation of 25-hydroxyvitamin D-1-hydroxylase and 24-hydroxylase in keratinocytes by PTH and FGF23. Exp. Dermatol. 2018, 27, 1201–1209. [Google Scholar] [CrossRef]
- Bejon, P.; Williams, T.N.; Liljander, A.; Noor, A.M.; Wambua, J.; Ogada, E.; Olotu, A.; Osier, F.H.; Hay, S.I.; Farnert, A.; et al. Stable and unstable malaria hotspots in longitudinal cohort studies in Kenya. PLoS Med. 2010, 7, e1000304. [Google Scholar] [CrossRef] [Green Version]
- Elliott, A.M.; Kizza, M.; Quigley, M.A.; Ndibazza, J.; Nampijja, M.; Muhangi, L.; Morison, L.; Namujju, P.B.; Muwanga, M.; Kabatereine, N.; et al. The impact of helminths on the response to immunization and on the incidence of infection and disease in childhood in Uganda: Design of a randomized, double-blind, placebo-controlled, factorial trial of deworming interventions delivered in pregnancy and early childhood [ISRCTN32849447]. Clin. Trials 2007, 4, 42–57. [Google Scholar] [CrossRef]
- Tiono, A.B.; Nebie, I.; Anagnostou, N.; Coulibaly, A.S.; Bowyer, G.; Lam, E.; Bougouma, E.C.; Ouedraogo, A.; Yaro, J.B.B.; Barry, A.; et al. First field efficacy trial of the ChAd63 MVA ME-TRAP vectored malaria vaccine candidate in 5–17 months old infants and children. PLoS ONE 2018, 13, e0208328. [Google Scholar] [CrossRef]
- Atkinson, S.H.; Rockett, K.; Sirugo, G.; Bejon, P.A.; Fulford, A.; O’Connell, M.A.; Bailey, R.; Kwiatkowski, D.P.; Prentice, A.M. Seasonal childhood anaemia in West Africa is associated with the haptoglobin 2-2 genotype. PLoS Med. 2006, 3, e172. [Google Scholar] [CrossRef] [Green Version]
- Nunes, M.C.; Cutland, C.L.; Jones, S.; Hugo, A.; Madimabe, R.; Simões, E.A.F.; Weinberg, A.; Madhi, S.A. Duration of Infant Protection Against Influenza Illness Conferred by Maternal Immunization. JAMA Pediatr. 2016, 170, 840–847. [Google Scholar] [CrossRef]
- Mogire, R.M.; Morovat, A.; Muriuki, J.M.; Mentzer, A.J.; Webb, E.L.; Kimita, W.; Ndungu, F.M.; Macharia, A.W.; Cutland, C.L.; Sirima, S.B.; et al. Prevalence and predictors of vitamin D deficiency in young African children. BMC Med. 2021, 19, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M.; Endocrine, S. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, A.C.; Manson, J.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: What clinicians need to know. J. Clin. Endocrinol. Metab. 2011, 96, 53–58. [Google Scholar] [CrossRef] [PubMed]
- WHO; CDC. Assessing the Iron Status of Populations: Report of a Joint World Health Organization/Centers for Disease Control and Prevention Technical Consultation on the Assessment of Iron Status at the Population Level, Geneva, Switzerland, 6–8 April 2004; World Health Organization and Centers for Disease Control: Geneva, Switzerland, 2005. [Google Scholar]
- World Health Organization. WHO Guideline on Use of Ferritin Concentrations to Assess Iron Status in Individuals and Populations; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Yamanishi, H.; Iyama, S.; Yamaguchi, Y.; Kanakura, Y.; Iwatani, Y. Total iron-binding capacity calculated from serum transferrin concentration or serum iron concentration and unsaturated iron-binding capacity. Clin. Chem. 2003, 49, 175–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Iron Deficiency Anaemia: Assessment, Prevention, and Control. A Guide for Programme Managers; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- WHO Multicentre Growth Reference Standard Group. WHO Child Growth Standards based on length/height, weight and age. Acta Paediatr. Suppl. 2006, 450, 76–85. [Google Scholar] [CrossRef]
- Jin, H.J.; Lee, J.H.; Kim, M.K. The prevalence of vitamin D deficiency in iron-deficient and normal children under the age of 24 months. Blood Res. 2013, 48, 40–45. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.A.; Hwang, J.S.; Hwang, I.T.; Kim, D.H.; Seo, J.H.; Lim, J.S. Low vitamin D levels are associated with both iron deficiency and anemia in children and adolescents. Pediatr. Hematol. Oncol. 2015, 32, 99–108. [Google Scholar] [CrossRef]
- Grindulis, H.; Scott, P.H.; Belton, N.R.; Wharton, B.A. Combined deficiency of iron and vitamin D in Asian toddlers. Arch. Dis. Child. 1986, 61, 843–848. [Google Scholar] [CrossRef]
- Sharma, S.; Jain, R.; Dabla, P.K. The Role of 25-Hydroxy Vitamin D Deficiency in Iron Deficient Children of North India. Indian J. Clin. Biochem. 2015, 30, 313–317. [Google Scholar] [CrossRef] [Green Version]
- Yoon, J.W.; Kim, S.W.; Yoo, E.G.; Kim, M.K. Prevalence and risk factors for vitamin D deficiency in children with iron deficiency anemia. Korean J. Pediatr. 2012, 55, 206–211. [Google Scholar] [CrossRef] [Green Version]
- Kaymak Cihan, M.; Unver Korgali, E. Is there an association between vitamin D level and iron deficiency in children? Arch. Argent. Pediatr. 2018, 116, e736–e743. [Google Scholar] [CrossRef] [PubMed]
- Abdul-Razzak, K.K.; Khoursheed, A.M.; Altawalbeh, S.M.; Obeidat, B.A.; Ajlony, M.J. Hb level in relation to vitamin D status in healthy infants and toddlers. Public Health Nutr. 2012, 15, 1683–1687. [Google Scholar] [CrossRef] [Green Version]
- Kang, Y.S.; Kim, J.H.; Ahn, E.H.; Yoo, E.G.; Kim, M.K. Iron and vitamin D status in breastfed infants and their mothers. Korean J. Pediatr. 2015, 58, 283–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houghton, L.A.; Trilok-Kumar, G.; McIntosh, D.; Haszard, J.J.; Harper, M.J.; Reid, M.; Erhardt, J.; Bailey, K.; Gibson, R.S. Multiple micronutrient status and predictors of anemia in young children aged 12–23 months living in New Delhi, India. PLoS ONE 2019, 14, e0209564. [Google Scholar] [CrossRef]
- Sato, H.; Takai, C.; Kazama, J.J.; Wakamatsu, A.; Hasegawa, E.; Kobayashi, D.; Kondo, N.; Nakatsue, T.; Abe, A.; Ito, S.; et al. Serum hepcidin level, iron metabolism and osteoporosis in patients with rheumatoid arthritis. Sci. Rep. 2020, 10, 9882. [Google Scholar] [CrossRef]
- Syed, S.; Michalski, E.S.; Tangpricha, V.; Chesdachai, S.; Kumar, A.; Prince, J.; Ziegler, T.R.; Suchdev, P.S.; Kugathasan, S. Vitamin D Status Is Associated with Hepcidin and Hemoglobin Concentrations in Children with Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2017, 23, 1650–1658. [Google Scholar] [CrossRef] [Green Version]
- Atkinson, S.H.; Armitage, A.E.; Khandwala, S.; Mwangi, T.W.; Uyoga, S.; Bejon, P.A.; Williams, T.N.; Prentice, A.M.; Drakesmith, H. Combinatorial effects of malaria season, iron deficiency, and inflammation determine plasma hepcidin concentration in African children. Blood 2014, 123, 3221–3229. [Google Scholar] [CrossRef] [Green Version]
- Doudin, A.; Becker, A.; Rothenberger, A.; Meyer, T. Relationship between serum 25-hydroxyvitamin D and red blood cell indices in German adolescents. Eur. J. Pediatr. 2018, 177, 583–591. [Google Scholar] [CrossRef] [PubMed]
- Malczewska-Lenczowska, J.; Sitkowski, D.; Surala, O.; Orysiak, J.; Szczepanska, B.; Witek, K. The Association between Iron and Vitamin D Status in Female Elite Athletes. Nutrients 2018, 10, 167. [Google Scholar] [CrossRef] [Green Version]
- Camaschella, C. Iron-deficiency anemia. N. Engl. J. Med. 2015, 372, 1832–1843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chowdhury, R.; Taneja, S.; Bhandari, N.; Strand, T.A.; Bhan, M.K. Vitamin D deficiency and mild to moderate anemia in young North Indian children: A secondary data analysis. Nutrition 2019, 57, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Zhong, S.; Liu, L.; Liu, S.; Li, X.; Zhou, T.; Zhang, J. Vitamin D deficiency and the risk of anemia: A meta-analysis of observational studies. Ren. Fail. 2015, 37, 929–934. [Google Scholar] [CrossRef] [PubMed]
- Kalach, N.; Benhamou, P.H.; Campeotto, F.; Dupont, C. Anemia impairs small intestinal absorption measured by intestinal permeability in children. Eur. Ann. Allergy Clin. Immunol. 2007, 39, 20–22. [Google Scholar] [PubMed]
- Braithwaite, V.; Prentice, A.M.; Doherty, C.; Prentice, A. FGF23 is correlated with iron status but not with inflammation and decreases after iron supplementation: A supplementation study. Int. J. Pediatr. Endocrinol. 2012, 2012, 27. [Google Scholar] [CrossRef] [Green Version]
- Braithwaite, V.S.; Mwangi, M.N.; Jones, K.S.; Demir, A.Y.; Prentice, A.; Prentice, A.M.; Andang’o, P.E.A.; Verhoef, H. Antenatal iron supplementation, FGF23, and bone metabolism in Kenyan women and their offspring: Secondary analysis of a randomized controlled trial. Am. J. Clin. Nutr. 2021, 113, 1104–1114. [Google Scholar] [CrossRef]
- Schouten, B.J.; Hunt, P.J.; Livesey, J.H.; Frampton, C.M.; Soule, S.G. FGF23 elevation and hypophosphatemia after intravenous iron polymaltose: A prospective study. J. Clin. Endocrinol. Metab. 2009, 94, 2332–2337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braithwaite, V.; Jarjou, L.M.; Goldberg, G.R.; Prentice, A. Iron status and fibroblast growth factor-23 in Gambian children. Bone 2012, 50, 1351–1356. [Google Scholar] [CrossRef] [Green Version]
- Cusick, S.E.; Opoka, R.O.; Lund, T.C.; John, C.C.; Polgreen, L.E. Vitamin D insufficiency is common in Ugandan children and is associated with severe malaria. PLoS ONE 2014, 9, e113185. [Google Scholar] [CrossRef]
- Muriuki, J.M.; Mentzer, A.J.; Kimita, W.; Ndungu, F.M.; Macharia, A.W.; Webb, E.L.; Lule, S.A.; Morovat, A.; Hill, A.V.S.; Bejon, P.; et al. Iron Status and Associated Malaria Risk Among African Children. Clin. Infect. Dis. 2018, 68, 1807–1814. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Wray, K.; Allen, A.; Evans, E.; Fisher, C.; Premawardhena, A.; Perera, L.; Rodrigo, R.; Goonathilaka, G.; Ramees, L.; Webster, C.; et al. Hepcidin detects iron deficiency in Sri Lankan adolescents with a high burden of hemoglobinopathy: A diagnostic test accuracy study. Am. J. Hematol. 2017, 92, 196–203. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant Characteristics | Overall | Kenya | Uganda | Burkina Faso | The Gambia | South Africa 9 |
|---|---|---|---|---|---|---|
| Total participants, n/total (%) | 4509 | 1361/4509 (30.2%) | 1301/4509 (28.9%) | 329/4509 (7.3%) | 629/4509 (13.9%) | 889/4509 (22.9%) |
| Median age in months (IQR) | 23.9 (12.3, 35.9) | 19.8 (12.7, 36.8) | 24.0 (23.9, 35.9) | 23.4 (19.7, 26.4) | 46.6 (35.2, 58.7) | 12.0 (11.9, 12.1) |
| Females, n/total (%) | 2216/4509 (49.1%) | 671/1361 (49.3%) | 641/1301 (49.3%) | 161/329 (48.9%) | 297/629 (47.2%) | 446/889 (50.2%) |
| Malaria parasitaemia 1, n/total (%) | 445/3293 (13.5%) | 227/1082 (20.8%) | 89/1280 (6.9%) | 64/303 (21.1%) | 65/628 (10.4%) | n/a |
| Inflammation 2, n/total (%) | 1019/4469 (22.8%) | 363/1344 (27.0%) | 306/1285 (23.8%) | 109/322 (33.9%) | 85/629 (13.5%) | 156/889 (17.6%) |
| Stunting, n/total (%) 3 | 581/2289 (25.4%) | 99/208 (47.6%) | 203/1282 (15.8%) | 103/307 (33.5%) | 176/492 (35.8%) | n/a |
| Underweight, n/total (%) 4 | 389/2487 (15.6%) | 102/389 (26.2%) | 103/1296 (8.0%) | 58/309 (18.8%) | 126/493 (25.6%) | n/a |
| Vitamin D Status 5 | ||||||
| Median 25(OH)D nmol/L (IQR) | 77.6 (63.6, 94.2) | 81.0 (66.3, 101.6) | 78.6 (65.1, 94.5) | 78.4 (64.5, 91.3) | 71.2 (59.1, 84.2) | 76.2 (60.6, 91.9) |
| 25(OH)D > 75 nmol/l | 2485/4509 (55.1%) | 815/1361 (59.9%) | 756/1301 (58.1%) | 186/329 (56.5%) | 265/629 (42.1%) | 463/889 (52.1%) |
| 25(OH)D 50–75 nmol/l | 1674/4509 (37.1%) | 464/1361 (34.1%) | 479/1301 (36.8%) | 123/329 (37.4%) | 302/629 (48.0%) | 306/889 (34.4%) |
| 25(OH)D <50 nmol/l | 350/4509 (7.8%) | 82/1361 (6.0%) | 66/1301 (5.1%) | 20/329 (6.1%) | 62/629 (9.9%) | 120/889 (13.5%) |
| 25(OH)D <30 nmol/l | 28/4509 (0.6%) | 4/1361 (0.3%) | 5/1301 (0.4%) | 0 (0%) | 2/629 (0.3%) | 17/889 (1.9%) |
| Iron Status 5 | ||||||
| Iron deficiency 6, n/total (%) | 1546/4399 (35.1%) | 491/1322 (37.1%) | 433/1240 (34.9%) | 115/319 (36.1%) | 134/629 (21.3%) | 373/889 (42.0%) |
| Iron deficiency anemia 7, n/total (%) | 661/2880 (23.0%) | 207/771 (26.9%) | 209/1182 (17.7%) | 96/304 (31.6%) | 107/623 (17.2%) | n/a |
| Anemia 8, n/total (%) | 1829/2971 (61.6%) | 556/793 (70.1%) | 623/1241 (50.2%) | 274/314 (87.3%) | 376/623 (62.4%) | n/a |
| Author, Year | Sample Size (n) | Country | Age | Population | Definition of Vitamin D Status | Markers Investigated | Findings |
|---|---|---|---|---|---|---|---|
| Iron Markers | |||||||
| Grindulis 1986 [31] | 145 | UK | 22 months | Asian children | VDD: <25 nmol/L | Serum iron, transferrin, ferritin and hemoglobin | Children with VDD had lower concentrations of hemoglobin and serum iron. No differences were observed with transferrin and ferritin levels. |
| Yoon 2012 [33] | 79 | South Korea | Median 1.8 (IQR 0.3–13) years | Children diagnosed with IDA | VDS: ≥75 nmol/L VDI: 30–75 nmol/L VDD: <30 nmol/L | Ferritin, serum iron and hemoglobin | No difference in ferritin, serum iron or hemoglobin levels in patients with VDS compared to those who had VDD or VDI. No correlation between vitamin D status and severity of anemia. |
| Jin 2013 [29] | 102 | South Korea | Range 3–24 months | Children attending hospital | VDS: ≥75 nmol/L VDI: 50–75 nmol/L VDD: <50 nmol/L | Ferritin and iron | Children with ID were four times more likely to develop VDI and VDD compared to those who were iron replete. 25(OH)D levels were not correlated with ferritin or iron levels. |
| Sharma 2015 [32] | 263 | North India | Range 3 months–12 years | Children attending outpatients | VDS: ≥75 nmol/L VDI: 30–75 nmol/L VDD: <30 nmol/L | Ferritin, serum iron and hemoglobin | The proportion of children with IDA was 66%, 49% and 25% in the VDD, VDI group and VDS groups, respectively. 25(OH)D levels were positively correlated with hemoglobin levels but not with ferritin or iron levels. |
| Cihan 2018 [34] | 117 | Turkey | 6 months–5 years | Children attending outpatients | VDS: ≥50 nmol/L VDI: 30–50 nmol/L VDD: <30 nmol/L | Serum iron, ferritin and hemoglobin | Maternal and child VDD was associated with ID/IDA in children. Children with ID/IDA had lower 25(OH)D levels than those without ID/IDA. Maternal/child 25(OH)D levels were positively correlated with hemoglobin levels in children. |
| Chowdhury 2019 [35] | 1000 | India | Range 0.5–2.5 years | Community-based children | VDD: <25 nmol/L | Hemoglobin and sTfR | Children with VDD were more likely to have anemia independently of ID. Hemoglobin levels were positively associated with 25(OH)D levels. Association between 25(OH)D and sTfR was not investigated. |
| Hemoglobin Only | |||||||
| Abdul-Razzak 2011 [35] | 203 | Jordan | Range 0.5–3 years | Infants and children attending primary care | VDS: ≥75 nmol/L VDI: <75 nmol/L VDD: <50 nmol/L | Hemoglobin | No difference in mean hemoglobin levels between vitamin D status categories (VDD, VDI and VDS). |
| Kang 2015 [36] | 70 | South Korea | Range 4–24 months | Mothers and their infants attending hospital | VDS: ≥75 nmol/L VDI: 50–75 nmol/L VDD: <50 nmol/L | Hemoglobin | Mothers and infants with anemia had lower 25(OH)D levels compared to those without anemia. |
| Houghton 2019 [37] | 120 | India | 12–23 months | Community-based children | VDD: <50 nmol/L | Hemoglobin | No association between 25(OH)D levels and anemia. |
| Houghton 2019 [12] | 500 | Kenya | 3–5 years | Preschool children | VDD: <50 nmol/L | Hemoglobin | 25(OH)D levels were positively correlated with hemoglobin levels. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mogire, R.M.; Muriuki, J.M.; Morovat, A.; Mentzer, A.J.; Webb, E.L.; Kimita, W.; Ndungu, F.M.; Macharia, A.W.; Cutland, C.L.; Sirima, S.B.; et al. Vitamin D Deficiency and Its Association with Iron Deficiency in African Children. Nutrients 2022, 14, 1372. https://doi.org/10.3390/nu14071372
Mogire RM, Muriuki JM, Morovat A, Mentzer AJ, Webb EL, Kimita W, Ndungu FM, Macharia AW, Cutland CL, Sirima SB, et al. Vitamin D Deficiency and Its Association with Iron Deficiency in African Children. Nutrients. 2022; 14(7):1372. https://doi.org/10.3390/nu14071372
Chicago/Turabian StyleMogire, Reagan M., John Muthii Muriuki, Alireza Morovat, Alexander J. Mentzer, Emily L. Webb, Wandia Kimita, Francis M. Ndungu, Alex W. Macharia, Clare L. Cutland, Sodiomon B. Sirima, and et al. 2022. "Vitamin D Deficiency and Its Association with Iron Deficiency in African Children" Nutrients 14, no. 7: 1372. https://doi.org/10.3390/nu14071372